|
|
||||||||||||||
|
A 40 year-old merchant, otherwise healty and without prveious complaints regarding his upper extremities, sustained a distal radius fracture of his non-dominant left wrist in October 1997 while playing soccer. The fracture was of the A type of the AO classification and involved disruption of the DRUJ and an ulnar styloid avulsion. Initial non-operative treatment at an outside institution resulted in malunion with foreshortening of 4 mm, a dorsal tilting of 40°and a radial tilting of 12° of the radius plateau and nun-union of the ulnar styloid. In January 1998, an other hand surgeon performed a corrective osteotomy utilizing a bone graft and a T-plate which was removed in November 1998.
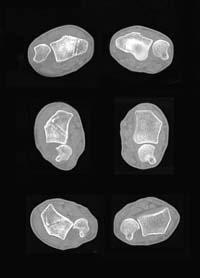
The patient presents with a very painful snapping at the DRUJ and frank palmar dislocation of the ulna versus the radius when the forearm is supinated past 30° of supination. There is tenderness over the ulnar styloid process. The DRUJ is tender and moderately unstable, both passively and actively. Pronation/supination encompass 80°/70°. Radioulnocarpal functions are reasonable, but the ranges of motion are shifted to 50° of flexion and 105° of extension with normal radial/ulnar deviation values. Grip strehngth measures 60 pounds. Other clinical findings are normal.
(1) What are your diagnoses? (2) Can you help the patient with non-operative means? (3) In case surgery was indicated, do you need additional information? Which one? |
||||||||||||||
| About Us | Research | Basic Knowledge | What's New | Forum | Guest Professor | Post a Case | eRadius Conference | Patients | Home |