|
|
||||||
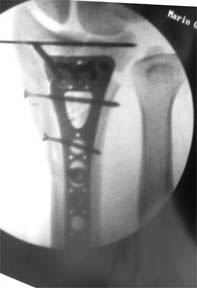
(case submitted August 10, 2007) Synopsis: 35 YO white male fell off his horse playing polo. A volar plate was applied, plus a K-wire and two 2.4 mm screws.
The subchondral screws are too proximal for optimum support. The K-wire was placed very distally, so as to not interfere with the screws. However, when the subchondral screws were placed, we placed them a bit proximal. It would be better to have the subchondral support screws more distally, but the fixation was solid (patient was 35) so the plate was not moved. The radius appears to be a bit overdistracted on the ulnar margin, but not on the radial margin. We believe that it is a bit overdistracted, but accepted the position, feeling that it will probably not be a problem, and revising the fixation would be. Better attention to this earlier would be nice, but it was a very difficult case, definitely requiring two surgeons. Overall, the articular reduction is excellent and the patient should do well (if we can keep him off his polo horse!) Each case teaches you something. This is what I learned from this challenging case: (1) Adequate incision. The tougher the case, the longer the incision and the wider the retraction. We were slowed down at first by not enough exposure distally. (2) Expand the exposure with each deeper layer of dissection. Do not let the dissection of each deeper layer decrease your exposure. (3) Debride the clot, callus, pre-pronator quadratus fat, and any torn fascia of the fibrous tissue of the fibrous transition zone. It will obscure your identification of the distal margin of the radius. (4) Identify what fragments you can; if you cannot see them all, check exposure and debridement. (5) Plan the reduction based on what you find. In general, assemble the articular fragments first and pin them. Remember, if the distal articular surface is dorsally tilted, you cannot use a PA view to assess your reduction. Tilt the mini-C arm as much as the distal fragment, so the facet view you obtain looks tangentially across the articular surface. (6) Stabilize the unstable shaft fragments with K-wires if their motion interferes with the progress of the reduction. (7) Place the plate in the approximately appropriate place on the distal fragment. Use the K-wire guides, screwed into the plate, to determine where the screws will go. Now is the time to assess the plate placement critically, before any screws are placed:
Move the plate mm by mm until you have an acceptable alignment. It is much harder or impossible to move the plate 1-2 mm if any screws have been placed. If in doubt about where a screw tip will be, leave the K-wire in place, remove the plate and guide, and get an end-on view of the K-wire. (8) Place the distal screws, checking screw length and placement vis-a-vis the articular surface, the radial styloid, and the dorsal ulnar corner of the radius, with fluoroscopy. 9) Reduce the dorsal tilt of the articular surface with the plate, the plate in place with one 3.5 mm shaft screw. Reassess everything. Then fill any remaining screw holes distally and proximally, if desired. (10) Assess all screws for length. The distal screws should be 3-4 mm short of the dorsal cortex. The proximal screws should be flush or no more than 1 mm proud. Thin patients can feel 2mm of pastpointing of the shaft screws. (11) Check the DRUJ. (12) Place the Marcaine block before closing, so you can be sure where the needle is. End of case. |
||||||
| About Us | Research | Basic Knowledge | What's New | Forum | Guest Professor | Post a Case | eRadius Conference | Patients | Home |