This is a talk given at the
American Society for Surgery of the Hand course
Hand and Upper Extremity Injuries
San Francisco November 2-3, 2001
External Fixation
for
Distal Radius
Fractures
David L. Nelson, MD
San Francisco, CA
I: History of External Fixation
A: Early History
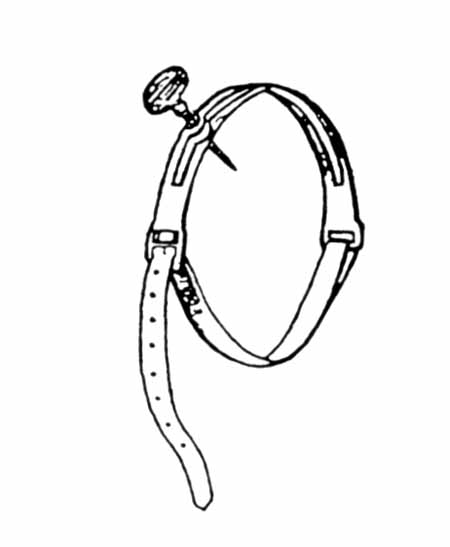
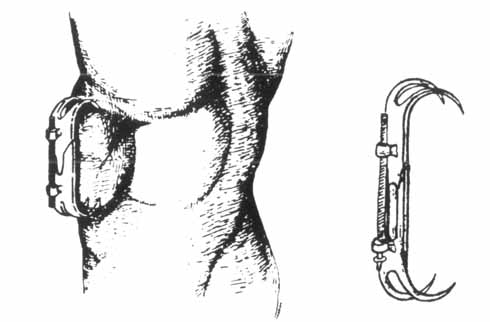
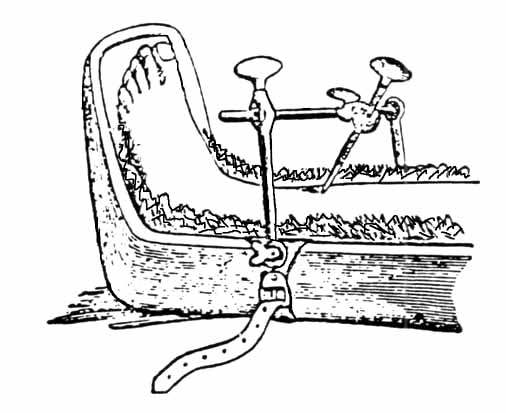
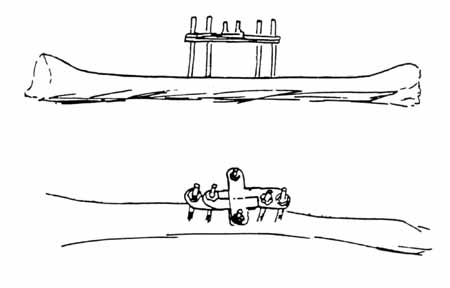
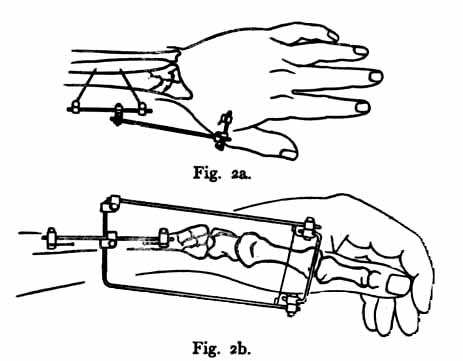
There are few things in surgery which are actually new, and this applies to external fixation. Hippocrates in about 400 BC wrote about a simple external fixator. The first use of "pins" is credited to Malgaigne who, in 1840, created a simple metal pin in a leather strap (Figure 1) for the percutaneous pin treatment of tibial fractures. He also made an external fixator for patella fractures he called a "griffe", or "claw." (Figure 2).
 |
 |
|
Figure 1 Malgaigne's pin |
Figure 2 Malgaigne's griffe |
Malgaigne's pin became popular, according to Burny (1965), and
was improved upon by others, including Bonnet, Deltheil, Roux (Figure 3), and
Ollier (Figure 4).
 |
 |
|
Figure 3 Roux's Device |
Figure 4 Ollier's Device |
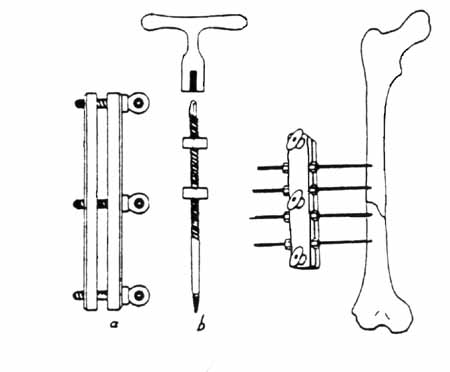
Parkhill in 1894 in the US treated fractures, nonunions, and malunions by threaded pins implanted into bone fragments and externally connected with two plates (figure 5).
 |
|
Figure 5 Parkhill's "bone clamp" |
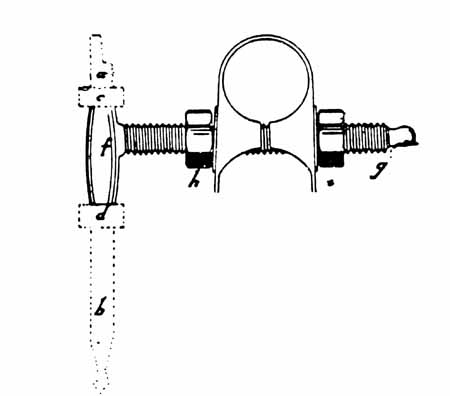
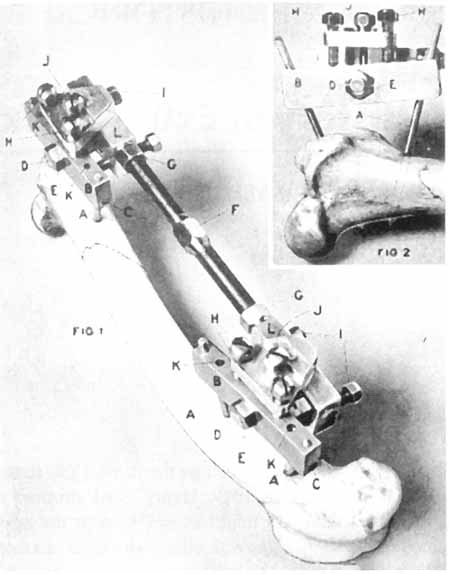
Lambotte, a Belgian surgeon, was the first to develop a device specially designed for external fixation, in 1902 (Figure 6). For the first time, the device allowed the placement of the pins in any needed direction and the pins were connected to the rod by adjustable clamps. The fracture had to be reduced prior to application of the external fixator. Lambotte is also credited with developing the first self-tapping threaded pin.
 |
 |
|
Figure 6 Lambotte's first external fixator |
Figure 7 Lambotte's adjustable pin |
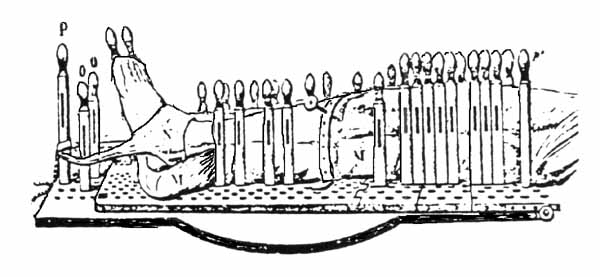
Shanz, Reidel, and Anderson used nails and screws in
conjunction with casts and developed the idea of non-parallel pins for firmer
control of bone fragments. The first adjustable external fixator was by Stader
(Figure 8) and was originally used in dogs, and the first adjustable external
fixator for the distal radius was by Roger Anderson in 1934 (Figure 9). The
Hoffmann external fixator came two years later in 1936.
 |
 |
|
Figure 8 Otto Stader's Splint |
Figure 9 Roger Anderson's fixator |
B Current Treatment
External fixation developed a bad reputation during the Second
World War, and many papers described the complications of the technique,
including pin infections, metacarpal fractures from pin holes, pin breakage or
loosening, nerve or tendon damage from pin insertion, and loss of reduction. As
external fixation technique matured, however, it went through many changes as
the various complications were addressed. The current techniques of external
fixation for the distal radius are based on the work of many people. Some of the
more important work is cited here.
Most authors who criticize external
fixation cite high complication rates (as high as 62%, Weber, 1986) but refer to
studies conducted prior to the above modifications. To continue to cite such
studies obscures the fact that current external fixation technique usually has a
very low complication rate. Schuind (1989) found only 9 complications in 225
cases; Weiland (1998) stated that there are "few major complications" with
current techniques of external fixation.
The most common "complication" currently is pin tract infection. However, since the wide adoption of requiring patient to shower with their fixator in place, the incidence of infections that require a change of treatment (e.g., pin removal) or decreased outcome for the patient are quite rare, and should be less than 1%. Minor pin tract infection, those that merely require more patient education or better compliance, or oral antibiotics, should be recognized for that they are: minor. As Margaret McQueen has stated, these are not "complications", they are "expected problems".
The major question remains whether external fixation or internal fixation yields a better range of motion for the unstable but reducible fractures, where either technique could be used. There are few prospective, randomized studies. Wright presented a study comparing these two techniques (ASSH Annual Meeting, 2001) and concluded that their range of motion was similar. Edwards (1991) found in a series of 30 patients with severely comminuted intra-articular fractures treated with external fixation, that the average ROM was 90% of the opposite side. Fernandez (1991) found in a series of forty patients with intraarticular distal radius fractures treated with external fixation that the ROM was 62 degrees of extension and 60 degrees of flexion. These studies compare quite favorably with studies of internal fixation. The final answer will lie with prospective, randomized studies.
In light of the current techniques of external fixation, where does this treatment fit in a modern treatment algorithm?
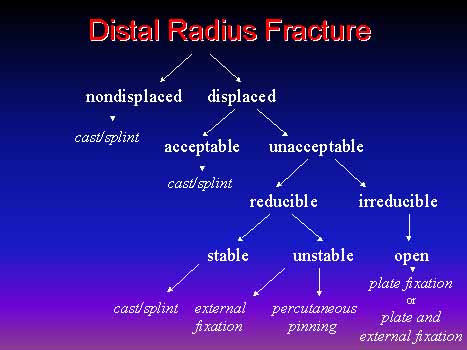
II: Treatment Algorithm for Distal Radius Fractures
A: General Algorithm
There is no one treatment algorithm that will be right for every surgeon and every patient. Each surgeon will have to decide what techniques work for him or her and when they should change from one technique to another. Here is my current algorithm.
B: The Crux of the Matter
When a fracture is unstable and needs operative treatment, the crux of the matter is deciding whether one should treat it with external fixation, accepting three to six weeks of immobilization, or open reduction and internal fixation, with the possibility of immediate mobilization. As noted in the previous section, there are few prospective studies and the answer is not yet clear. Both treatment groups seem to have similar outcomes in terms of range of motion, with external fixation possibly having fewer complications with current technique.
III: Current External Fixation
Technique
A Lidocaine block
There is scientific evidence that placing a pre-incision block of 2% Lidocaine will decrease the amount of anesthetic that is required during the early part of the procedure and may decrease post-operative pain (see http://www.PeriOperativePain.com for further information). Place the Lidocaine into the sites of pin placement, both superficial and deep (periosteum), and into the fracture site.
B Initial pinning
If there is a non-displaced intraarticular fracture, pinning with two .045 inch K-wires, prior to any initial manipulation, will prevent displacement of the intra-articular component.
C Initial reduction
An initial reduction should be performed prior to placing the external fixator. This decreases skin tension, helps planning the placement of the pins, and assesses the fracture mobility if the fracture has had some time to heal.
D Pin placement
The only pin that is uniquely positioned is the proximal second metacarpal pin. Options include placement in the metaphysis or the diaphysis. Diaphyseal pin engagement into two cortices works well, with no need to go into the third metacarpal, which can cause injury to the intervening interosseous muscles.
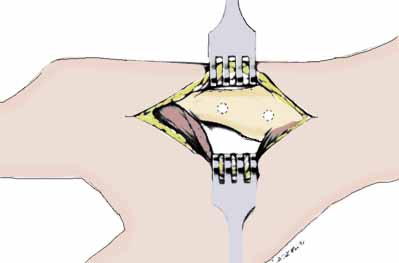
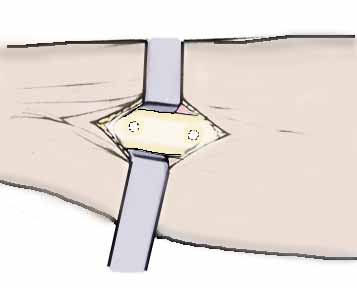
E Open placement
The pins should be placed through small open incisions (Seitz, 1990). The incision should be large enough to allow good visualization of the cutaneous nerves and interosseous muscles, and to allow placement of the pin into the center of the bone. Open section pin placement must be avoided. It would be difficult to defend a nerve injury, or metacarpal or radial fracture due to inadequate visualization from the use of a stab incision, as the technique of open placement is well established and the complications are well described.
F 45° placement of pins
Some fixator design (e.g., the Agee WristJack) require pin placement in the coronal plane. If the fixator design permits, pins should generally be placed 45° to the sagittal plane, that is, halfway between the sagittal and the coronal planes. The metacarpal pins are placed dorsal to the interosseous muscle and volar to the extensor mechanism. The radius pins are placed between the ECRL and the ECRB, or alternatively, between the ECRB and the EDC (technique of Hill Hastings). Placement of the pins in the straight lateral plane places the pins in very close proximity to the radial sensory nerve.
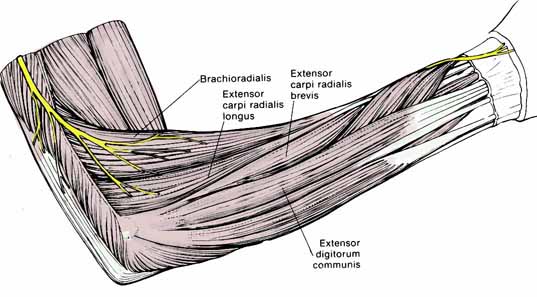
In a study in our lab using 10 cadavers, the distance from the radial sensory nerve and the site of pin placement was measured for various intermuscular intervals. If pins were placed between the BR and ECRL, they were an average of 4.8 mm (range 0-14 mm) from the RSN at the proximal end of the interval; at the distal end of this interval, they typically were at or into the nerve. If the pins were placed into the ECRL-ECRB interval, they were an average of 11 mm (range 6-20 mm) proximally to 5 mm (range 0-11 mm) distally from the RSN. The nerve was always separated from the pins by the muscle and tendon of ERCL. If the pins were placed between the ECRB and EDC, they were at least 10 mm from the nerve.
A welcome side effect of this is that this forces the fixator to be out of the plane of the lateral xray. Use of a radiolucent fixator obviates most of this advantage, but is still the preferred plane of fixator placement.
G Proximal pin placement
The fixator should be used as a template to define the most distal and most proximal possible sites for pin placement. The proximal pins are placed with open technique at 45°. Once all the pins are placed, their position should be checked with fluoroscopy.
H Fixator choice
Any fixator currently on the market probably can be used effectively. The technique of device placement and surgical decision-making are more important than the brand of fixator. All devices are capable of multiplanar ligamentotaxis, and most brands have one model that is radiolucent. The most important characteristic in a fixator is that you are comfortable with it and it fits your style and approach to distal radius fracture management. Cost is increasingly important and should not be ignored. The uniplanar tube style of fixator with multiaxial joints (usually ball joints) provides more rigidity and ease of changing position than the earlier rods-and- connectors style of devices, such as the Roger Anderson, Hoffman, Ace Colles, or early AO fixators. Some fixators will allow controlled adjustments in the office or clinic, without need for anesthesia. With other designs, adjustment may be difficult without anesthesia. However, in skillful hands, any style of fixator can be used.
I Fracture reduction
Temporary over-distraction may be used intraoperatively, but final distraction should be checked with fluoroscopy. The radioscaphoid distance should, in general, not be more than 1 to 2 mm larger than normal. K-wire "joy sticks" can be used if necessary for percutaneous manipulation of fragments.
J Percutaneous pins
Once the reduction is obtained, percutaneous pins are often added for additional stability. Wolfe (1999) has shown that K-wire augmentation demonstrated a significant reduction in motion of the distal radial fragment of at least 40% in all 3 rotational planes, that the addition of the single dorsal K-wire significantly improved stability regardless of the type of external fixator that is used.
K Bone graft
Most authors recommend bone grafting if the reduction has left a void in the radial metaphysis, especially if the fracture has been opened for any other reason (ie, open manipulation of a fracture fragment).
L Wrist position and finger ROM
If the wrist is immobilized in flexion (the now- discontinued Cotton-Loder position), the fingers will not be able to fully flex and finger stiffness will result. In addition, Gelberman (1984) has shown that the flexed posture will create acute median nerve compression in distal radius fracture patients who otherwise would not have a problem.
M DRUJ stability
It is important to check DRUJ stability once the radius fracture is stabilized. If needed, place a .062 inch K-wire across the DRUJ, proximal to the joint. Consider ORIF of large ulnar styloid fragments if present.
N Marcaine
A Marcaine block at the end of the procedure will dramatically reduce the need for post-operative pain medication. In a prospective, 2-yr study of all the hand surgery patients in a single private practice, 49.6% of the patients did not require any post-operative pain medication (see http://www.DavidLNelson.MD/PostOperativePain.htm).
O Hand therapy
The patient needs to be started on a program of finger, elbow, and shoulder range of motion. If they cannot do it themselves, referral for formal hand therapy should be done. This decision can often be made, and the referral sent, prior to surgery.
P Fixator removal
In the decade of the 1980's, fixators were commonly left in place for eight weeks. This time period has progressively shortened, with six weeks being the most common time period, but many have good experience with shorter time periods. Bone grafting of the radius fracture can allow earlier fixator removal.
Q Median nerve decompression
Median nerve dysfunction in the setting of an acute distal radius fracture is not carpal tunnel syndrome; it is acute median nerve compression, often complicated by nerve contusion. These should not be confused. The former is low pressure over a long period of time; the latter is high pressure over a short period of time. It has been widely suggested that the nerve be decompressed if the patient is taken to the operating room for treatment (McCarroll, 1984, Jupiter, 1991).
![]()
References & Bibliography
Agee JM. Distal radius fractures. Multiplanar ligamentotaxis. Hand
Clin. 1993 Nov;9(4):577-85.
Axelrod TS, McMurtry RY. Open reduction and
internal fixation of comminuted, intraarticular fractures of the distal radius.
J Hand Surg [Am]. 1990 Jan;15(1):1-11.
Burny F. Implants en chirurgie osseuse. Appercu historique. Actsa Orthop Belg 40: 563-609, 1974. Cited in Schuind F. A short history of external fixation. In: Complex Distal Radius Fractures, Nelson D, ed., 1994.
Cooney WP 3rd, Dobyns JH, Linscheid RL. Complications of Colles' fractures. J Bone Joint Surg Am. 1980;62(4):613-9.
Edwards GS Jr. Intra-articular fractures of the distal part of the radius treated with the small AO external fixator. J Bone Joint Surg Am. 1991 Sep;73(8):1241-50.
Fernandez DL, Geissler WB. Treatment of displaced articular fractures of the radius. J Hand Surg [Am]. 1991 May;16(3):375-84.
Gelberman RH, Szabo RM, Mortensen WW. Carpal tunnel pressures and wrist position in patients with Colles' fractures. J Trauma. 1984 Aug;24(8):747-9.
Jupiter JB. Fractures of the distal end of the radius. J Bone Joint Surg Am. 1991 Mar;73(3):461-9.
McCarroll HR Jr. Nerve injuries associated with wrist trauma.
Orthop Clin North Am. 1984 Apr;15(2):279-87.
Price C. External fixation.
Proceedings of the International Riva Conference, Riva, Italy, 1992.
Schuind F, Donkerwolcke M, Rasquin C, Burny F. External fixation of fractures of the distal radius: a study of 225 cases. J Hand Surg [Am]. 1989 Mar;14(2 Pt 2):404-7.
Seitz WH Jr, Putnam MD, Dick HM. Limited open surgical approach for external fixation of distal radius fractures. J Hand Surg [Am]. 1990 Mar;15(2):288-93.
Weber SC, Szabo RM. Severely comminuted distal radial fracture as an unsolved problem: complications associated with external fixation and pins and plaster techniques. J Hand Surg [Am]. 1986 Mar;11(2):157-65.
Weiland, A. Fractures of the Distal Radius, 1998; 67-82. In: Levine A, ed: Orthopedic Knowledge Update: Trauma. AAOS, Rosemont, Illinois.
Smith D, Wright T: Outcome study of unstable distal radius fractures: ORIF with a volar fixed angled tine plate vs external fixation. ASSH Annual meeting, October 2-6, 2001, Baltimore, Maryland. http://assh.confex.com/assh/2001/finalprogram/abstract_712. htm.
Wolfe SW, Austin G, Lorenze M, Swigart CR, Panjabi MM. A biomechanical comparison of different wrist external fixators with and without K-wire augmentation. J Hand Surg [Am]. 1999 May;24(3):516-24.